Wisdom teeth — the third molars — are the most frequently extracted teeth in dentistry. Approximately five million Americans have their wisdom teeth removed each year. Yet a significant number of those extractions are performed on teeth that are not currently causing any symptoms. This raises a reasonable question: if they are not hurting, why remove them?
The answer depends on a careful evaluation of impaction status, available space, relationship to adjacent structures, and patient age and history. Here is a candid breakdown of the evidence — including when removal is clearly warranted, when it is clearly not, and when the decision genuinely requires individual evaluation.
Why Wisdom Teeth Are So Often Problematic
Wisdom teeth typically erupt between ages 17 and 25. The human jaw, over evolutionary time, has been shrinking — the result of dietary changes that no longer require the robust chewing apparatus of our ancestors. The third molars, however, have not disappeared. They attempt to erupt into a jaw that often lacks adequate space to accommodate them, resulting in impaction.
An impacted wisdom tooth is one that is blocked from fully erupting by adjacent teeth, bone, or soft tissue. Impaction can be partial (partially erupted, partially covered by gum) or complete (entirely within the bone). Four types of impaction are described by orientation: vertical, horizontal, mesioangular (tilted forward toward the second molar), and distoangular (tilted backward).
When Removal Is Clearly Indicated
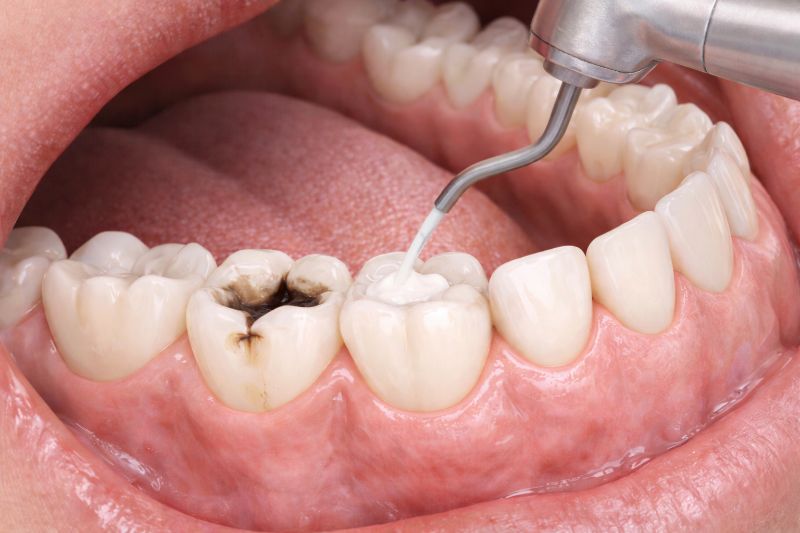
Active infection (pericoronitis). When a wisdom tooth partially erupts, the gum flap covering it creates a pocket that is impossible to clean. Food and bacteria accumulate, causing recurring infection of the surrounding tissue. Pericoronitis is painful, can spread, and recurs until the tooth is removed.
Decay. Partially erupted wisdom teeth are nearly impossible to clean properly with a toothbrush. Cavities develop in the wisdom tooth itself and — critically — on the back surface of the adjacent second molar. Second molar cavities caused by wisdom tooth proximity are a well-documented and clinically significant complication.
Damage to adjacent teeth. Mesioangularly impacted wisdom teeth (angled forward) exert direct pressure on the second molar root, potentially causing root resorption — irreversible destruction of the second molar’s root. This finding on X-rays is an unambiguous indication for removal.
Cyst formation. An unerupted tooth is enclosed in a follicular sac. This sac can expand into a dentigerous cyst — a fluid-filled cavity within the jawbone. If untreated, large cysts can cause jaw fracture, displace other teeth, and require more extensive surgical treatment to remove.
Pain and pressure. Symptomatic impacted wisdom teeth causing persistent discomfort are a straightforward indication for extraction.
When Removal Is Not Clearly Necessary
Fully erupted, functional third molars in adequate space. If a wisdom tooth has erupted completely, is correctly positioned to function in the bite, has an opposing tooth to occlude with, and can be cleaned effectively with a toothbrush, it is a normal tooth. There is no evidence-based justification for extracting a healthy, functional wisdom tooth.
Deeply impacted teeth in older patients with no pathology. The American Academy of Oral and Maxillofacial Surgeons acknowledges that in adults over 35–40 with fully bony impactions and no radiographic evidence of pathology (no decay, no cyst, no resorption), a monitoring approach with periodic radiographic surveillance is a reasonable alternative to prophylactic extraction — particularly given the increased surgical risks in older patients.
The Age Factor
Wisdom teeth are easiest to remove between the ages of 17 and 25, when roots are incompletely formed, the bone is more flexible, and healing is faster. Waiting until the roots are fully developed and the bone is more dense increases surgical complexity, risk of nerve proximity complications, and recovery time.
This is why many oral surgeons and dentists recommend evaluation — and extraction when indicated — during the late teenage years rather than waiting for symptoms to develop. Early intervention, when warranted, is generally safer and recovers faster than late intervention after complications arise.
What Monitoring Looks Like
For patients whose wisdom teeth do not clearly require removal, monitoring involves: panoramic X-ray every 1–2 years to assess for developing pathology, clinical examination for signs of pericoronitis or periodontal involvement, and regular assessment of adjacent second molar health.
The monitoring approach is appropriate only when there is active dental care with reliable follow-through — not as justification for indefinite avoidance of evaluation.
What to Expect if You Do Have Them Removed
Wisdom tooth removal under local anesthesia or sedation is one of the most routinely performed oral surgery procedures. Most patients manage the post-operative period — typically 3–7 days of swelling, soreness, and a soft food diet — comfortably with prescribed or over-the-counter pain medication and cold compresses. Dry socket (alveolar osteitis), the most common complication, occurs in 2–5% of extractions and is easily managed.
Serious complications — nerve injury, jaw fracture — are rare but real, particularly for deeply impacted lower wisdom teeth in close proximity to the inferior alveolar nerve. Reviewing your 3D or panoramic imaging with your surgeon and understanding the specific anatomy of your case is an important step before consenting to surgery.
My Recommendation
Get a proper evaluation — ideally a panoramic X-ray — during your late teens or early twenties if you have not already. Let the anatomy, impaction status, and clinical findings guide the decision. Do not remove wisdom teeth that are healthy, erupted, and functional. Do not keep wisdom teeth that are causing disease, damaging adjacent teeth, or clearly at high risk of doing so. And make the decision early, when options are most favorable, rather than waiting for an acute episode to force the issue under less ideal circumstances.