Dry mouth — or xerostomia — is far more than a minor discomfort. It is a significant medical condition that, when persistent, creates conditions in the mouth that dramatically accelerate tooth decay, promote gum disease, make swallowing and speaking difficult, and substantially reduce quality of life. It affects an estimated 40 million Americans, most of whom are managing it inadequately.
What Saliva Actually Does
Saliva is one of the body’s most underappreciated fluids. A healthy adult produces approximately 1 to 1.5 liters of saliva per day. During waking hours, this constant flow performs several critical functions simultaneously:
Acid neutralization. After eating, the mouth becomes acidic. Saliva contains bicarbonate buffers that neutralize this acid within minutes, preventing prolonged enamel exposure.
Remineralization. Saliva is supersaturated with calcium and phosphate — the minerals that make up enamel. This mineral-rich environment continuously replenishes enamel that is being dissolved by dietary acids.
Antimicrobial action. Salivary proteins including immunoglobulins, lysozyme, and lactoferrin directly suppress cavity-causing and gum disease-causing bacteria.
Mechanical cleansing. The constant flow of saliva washes food particles and bacteria from tooth surfaces and carries them toward the stomach.
When saliva production drops significantly, every one of these protective mechanisms is compromised simultaneously. The result is a marked acceleration of dental disease.
What Causes Dry Mouth?
Medications — by far the most common cause. More than 400 commonly prescribed medications list dry mouth as a side effect, including antihistamines, antidepressants (SSRIs, TCAs), antihypertensives (diuretics, beta-blockers, ACE inhibitors), anticholinergics (bladder medications, anti-nausea drugs), opioids, and benzodiazepines. Polypharmacy — taking multiple medications simultaneously — compounds the effect dramatically.
Age. Dry mouth is not a direct consequence of aging — it is a consequence of the higher medication burden carried by older adults. However, salivary gland function does decline modestly with age and systemic disease.
Sjögren’s syndrome. An autoimmune condition in which the immune system attacks the salivary and lacrimal (tear) glands, causing severe dry mouth and dry eyes. Affects approximately 4 million Americans, predominantly women, and is frequently underdiagnosed.
Radiation therapy to the head and neck. High-dose radiation for head and neck cancers can permanently damage salivary gland tissue, causing severe and lasting xerostomia.
Diabetes. Poorly controlled blood glucose is associated with reduced salivary flow, altered salivary composition, and increased susceptibility to oral infections.
Mouth breathing. Habitual mouth breathing — often due to nasal obstruction, allergies, or sleep apnea — dries oral tissues and disrupts the protective salivary film on tooth surfaces, particularly during sleep.
Dehydration and lifestyle. Insufficient water intake, high caffeine and alcohol consumption, and smoking all contribute to reduced salivary flow.
The Dental Consequences
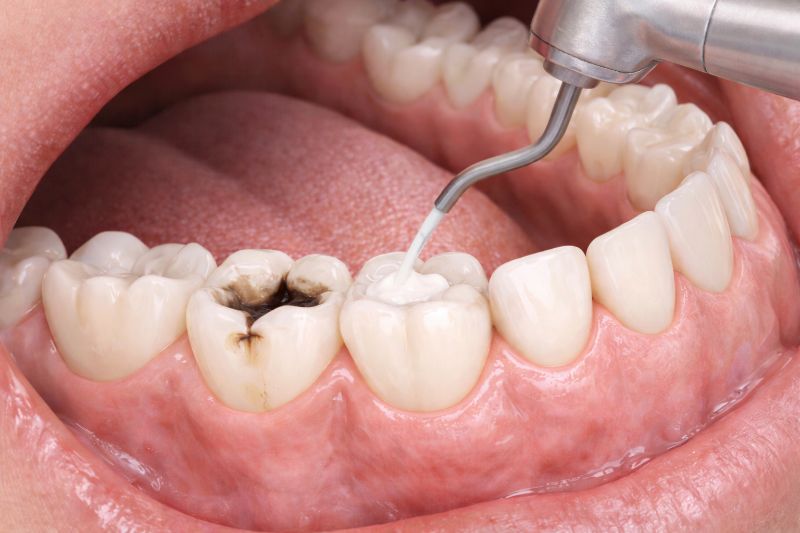
Patients with significant dry mouth experience dramatically accelerated dental deterioration. A pattern I see repeatedly: a patient who maintained healthy teeth for decades begins taking a new medication, reduces their water intake, and within 12–18 months has developed multiple new cavities — often in atypical locations like root surfaces and near the gumline, which are characteristic of xerostomia-related decay.
The mechanism is straightforward: without adequate saliva to neutralize acid and remineralize enamel, dietary acid exposure causes cumulative damage that is never repaired.
Treatment Options
Increase water intake. Drink water throughout the day — not just at meals. Carry a water bottle and sip consistently. This is the simplest and most universally available intervention.
Stimulate saliva flow. Chewing sugar-free gum sweetened with xylitol stimulates the salivary reflex and provides the added benefit of xylitol’s cavity-protective properties. Xylitol lozenges and mints are an alternative for patients who prefer not to chew gum.
Saliva substitutes. Over-the-counter products including Biotene Oral Balance gel, ACT Dry Mouth lozenges, and OralMoist discs replace some salivary function by providing lubricating polymers and minerals. They do not replicate natural saliva but provide meaningful symptomatic relief, particularly at night.
Prescription medications. Pilocarpine (Salagen) and cevimeline (Evoxac) are cholinergic medications that directly stimulate the salivary glands in patients who retain residual gland function. They are particularly effective in Sjögren’s syndrome and post-radiation xerostomia. Both require a prescription and should be used under medical supervision.
Address the underlying cause. Discuss the medication side effect list with your prescribing physician. Switching to an alternative medication with a lower xerostomic profile — where clinically appropriate — can significantly reduce dry mouth severity. Do not stop prescribed medications without consulting your physician.
Prescription fluoride. For patients with active xerostomia, I recommend 5,000 ppm prescription fluoride toothpaste (PreviDent, Clinpro 5000) used in place of standard toothpaste nightly. The higher fluoride concentration provides continuous remineralization that partially compensates for reduced salivary mineral delivery.
Night guard. For mouth breathers, a simple nighttime appliance or nasal breathing aid can reduce overnight desiccation of oral tissues. Addressing the underlying nasal obstruction is the more complete solution.
A Note on Mouthwash
Most commercial mouthwashes contain significant concentrations of ethanol (alcohol), which worsens dry mouth by further desiccating oral tissues. Patients with xerostomia should use only alcohol-free rinses — specifically those formulated for dry mouth, such as Biotene Dry Mouth Oral Rinse or ACT Dry Mouth Rinse.
When to Tell Your Dentist
If you are experiencing dry mouth, tell your dentist even if you consider it mild or attribute it to a medication you take. We need to adjust your recall interval, apply professional fluoride at every appointment, and monitor for the early signs of xerostomia-related decay that can be reversed if caught before it progresses. We can also help you build a comprehensive management protocol that addresses the specific causes and severity of your dry mouth.
Dry mouth is manageable. But like most things in oral health, managing it effectively requires acknowledging the problem and addressing it systematically — not hoping it improves on its own.